| Macular Degeneration (ARMD) |
 |
|
|
| |
| |
Age Related Macular
Degeneration (ARMD) is degeneration of the most
sensitive part of the retina (sensory part of the
eye) called macula. It is mostly seen in people over
the age of 50 years.
Initially it is a silent disease and can affect one
eye to begin with. At this stage it might be
detected by an ophthalmologist on routine retina
evaluation. Gradually vision loss increases mainly
in the center allowing vision at sides, but makes
reading or close work difficult without the use of
special low vision aids.
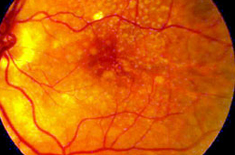
The early stages of ARMD typically start with
appearance of deposits beneath the retina called
Drusen. These do not affect vision very much by
themselves and most people with Drusen will never
have a serious loss of vision. However, certain
changes may occur that lead to the late stage of
ARMD which leads to marked visual loss. |
 |
What Causes it and Who is at Risk ? |
| |
The exact cause of
macular degeneration is not known though
following risk factors have been identified:
age, heredity, sex (women more affected then
men), light ocular pigmentation,
hypertension, cardiovascular diseases,
diabetes, photo toxicity and cigarette
smoking.
Types: There are 2 types of ARMD:
“Dry” and “Wet”
Dry ARMD is the most common form
accounting 80-90% of all cases and is
associated with ageing. It is caused by
degeneration in visual cells leading to
yellow-white deposits in layers of retina
called drusen or formation of atrophic areas
in macula. Overtime dry ARMD may develop
into wet type.
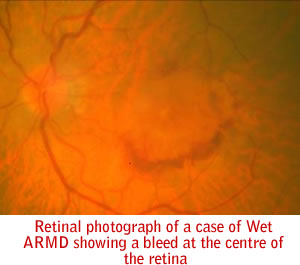
Wet or Exudative ARMD is the more
severe variety where abnormal blood vessels
form beneath the macula which leak fluid and
blood under the retina. Blood under the
retina is toxic to the photoreceptors and
can lead to severe loss of function of
retina. |
|
What are the signs & symptoms? |
| |
If only one eye is
affected to begin with, the symptoms may not
be noticeable in early stages. Gradually as
disease progresses or if both eyes are
involved, reading or close work may become
difficult. Common symptoms are distortion of
objects which are looked at directly, for
e.g. bulges or curved appearance of a
straight door, distorted print lines in book
(metamorphopsiae), missing of letters
or words while reading, a dark or blank spot
in the center of vision, (scotoma) or
fading of colors specially blue (dyschromatopsiae) |
|
How is it diagnosed? |
| |
As initially it is a
silent disease, mostly it is picked up in a
routine retina examination by an
ophthalmologist .The retinal examination
done by an ophthalmoscope will show the
findings of this disease process. To assess
the condition in detail, certain other test
are done:
-
Amsler
Grid: It is a test paper with
graphic picture to be used at reading
distance with near glasses on. This is
used to check for extent of sight
loss-dark spot, distortion or missing of
straight lines and also is given to the
patient to take home so that he can
monitor his symptoms at home and report
immediately if there is worsening.
-
Fundus
Fluorescin Angiography (FFA) /
Indocyanine Green Angiography (ICG):
the photographs of macula are taken
after injecting a dye in patient’s arm.
The dye reaching the eye helps to
clarify the type and extent of disease,
including detail of abnormal vessels,
leaks and membrane formations.
-
Optical
Coherence Tomography (OCT) : In this
test photographs of the retina are taken
to show its microscopic detail. So it
can help detect any early thickening of
the retina in wet ARMD. Also it can
delineate the abnormal blood vessels (
choroidal neovascularisation ) from
where the blood oozes. Changes of dry
ARMD such as drusen can also be
demonstrated. Also it is an excellent
tool to follow up after treatment to
assess the effect of the treatment done
and need for re-treatment.
|
|
How can it be prevented? |
| |
There is no
prevention of ARMD. Early detection is the
key to prevent severe loss of vision. All
individuals above 50,especially if there is
a family history of ARMD, history of
cardiovascular disease, light ocular
pigmentation, should get annual retinal
check up for the same. Anyone experiencing
following symptoms should consult an
ophthalmologist immediately:
Smoking is a risk
factor and should be avoided at all costs if
any of the risk factor is present.
According to some recent international
multicentric trials, multivitamins may slow
down progression of dry ARMD. However,
excess of fat soluble multivitamins can have
their own side-effects and thus consult your
doctor before regularly taking multivitamin
pills.
|
|
What is the treatment? |
| |
Dry ARMD
There is no
permanent cure for dry ARMD. The aim of
management is to keep a vigilant check on
progression of disease and take measures to
improve functional capability of the
patient.
-
Nutrition: Eat
fresh fruits, dark green leafy
vegetables. The role of
antioxidants/zinc in retarding the
progression is not very clear but
supplementation with Vitamins A, C and
E, zinc and selenium may have a positive
effect. A multicentric international
trial has demonstrated that
Multivitamins slow progression of
moderate dry ARMD to severe dry ARMD.
-
Sunlight: Blue
rays of the spectrum seem to accelerate
macular degeneration. Sunglasses with
good UV filters for outdoor activities
are recommended.
-
Smoking: quit
smoking as this accelerates the process
of ARMD
-
Early detection:
Monitoring of vision by Amsler Grid
-report immediately to eye surgeon if
any change noticed (the development of
wet type may need urgent treatment)
-
Low vision aids
and lighting – These are devices, which
can improve quality of living by
improving vision for day-to-day
activities, specially reading. Special
optical devices like magnifiers (hand
held, desktops or in spectacles) can be
used in various ways. Adequate lighting
will make reading more comfortable with
50-watt indoor bulb in metal shade then
fluorescent light.
Wet ARMD
The mainstay of treatment of wet ARMD at
present is injection of Anti-VEGF drugs into
the eye. These are special molecules
designed to stop further development of
blood vessels. So once the abnormal vessel
growth under the retina gets inhibited the
leakage of fluid and blood also reduces.
However at present these injections need to
be repeated at regular intervals as once the
effect of the drug wanes off the abnormal
vessels star growing again. The two main
such drugs being used at present are AVASTIN
& LUCENTIS. Presently we donot have a drug
which can altogether end the process of this
abnormal neovascularisation. A lot of
research is ongoing to find a permanent cure
for ARMD.
Other treatment modalities available for wet
ARMD are -
Photodynamic therapy (PDT) – This
involves treating the abnormal vessels with
a LASER after injecting a dye which
selectively enhances LASER energy absorption
by the new vessels only thus preventing
damage to the overlying retina. This therapy
also may be required to be repeated upto 3
times or more. International studies using
this dye have found it to prevent further
loss of vision in many cases but it is also
not hundred percent effective. Also it does
not improve vision but aims to stabilise it,
whereas the anti-VEGF injections can improve
vision also.
Conventional Laser treatment-This procedure
uses a high-energy laser beam to destroy the
fragile leaking blood vessels. This will
also not improve vision but may reduce
further progressive vision loss. However
since the high energy laser also destroys
retina, it can only be done for lesions away
from the central most sensitive part of the
retina.
Combinations treatments combining anti-VEGF
injections, intraocular steroid injections
and PDT are also being tried in some cases. |
| |
|
|
| |
Author: uthor: Dr. Rohan Chawla
Last updated on: 28 November 2008 |
| |
|
|
|
