|
What is it? |
| |
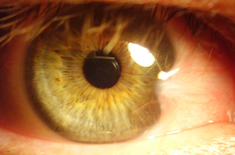
It is a degenerative condition of the sub-conjunctival tissue, which proliferates as
a triangular fold of tissue-mass to invade the cornea, involving the bowman,s membrane
and the superficial stoma, the whole thing being covered by conjunctival epithelium.
Literally , it means a wing. |
|
What Causes it? |
| |
It's not clear what causes a pterygium to develop. But most experts believe that
significant risk factors include:
Prolonged exposure to ultraviolet light
Dry eye
Irritants such as dust and wind
Pterygium occurrence is much greater among people who live near the equator. But it
also can develop in anyone who lives in a sunny climate. It's most often seen in young
adults ages 20 to 40. It appears to be more common in men than in women.
Pterygium is often preceded by a related non cancerous condition called pinguecula (pin-
WEK-yoo-la). This is a yellowish patch or bump on the conjunctiva near the cornea. The
conjunctiva is the thin, moist membrane on the surface of the eye. |
|
Who are at risk? |
| |
Ans3-Risk factors for pterygium include:
Work in occupations with excessive exposure to environmental conditions (sunlight, dust,
dirt, heat, dryness, wind, smoke)
Work in occupations with excessive exposure to solvents or chemicals
Family members with pterygium. |
|
What are the symptoms & signs? |
| |
The signs of pterygium is based on the clinical appearance of the lesion. Typical
findings include
1. Fibrovascular conjunctival growth within the palpebral fissure extending onto the
corneal surface
2. Triangular shape with the apex, or head, extending onto the cornea
3. Vascular straightening in the direction of the advancing head of the pterygium on the
corneal surface.
4. May be a thin translucent membrane or significantly thickened with an elevated mound
of gelatinous material.
5. It may affect the nasal and temporal limbus of both eyes or only a single location.
6. Raised lesion, white to pink in color depending on vascularity
7. Ranges from a fine transparent area with very mild elevation, few vessels, and minimal
corneal involvement in the early stages to a thick opaque vascular growth extending to
the visual axis in later stages
Pinguecula are often present in the ipsilateral or contralateral eye
A pigmented epithelial iron line (Stockers line) adjacent to a pterygium is evidence of
chronicity.
It is unusual for pterygia to deviate from the characteristic locations of three and nine
oclock within the palpebral fissure. Pterygioid lesions in other locations should elevate
suspicion for alternate diagnoses.
Symptoms
In some cases, a pterygium can grow onto the cornea (the clear, outer layer of the eye).
This can distort the shape of the cornea, causing a condition called astigmatism. The
result can be blurred vision.Symptoms of pterygium may include:
Burning
Gritty feeling
Itching
Sensation of a foreign body in the eye
Blurred vision. |
|
How is it diagnosed? |
| |
A physical examination of the eyes and eyelids confirms the diagnosis. Special
tests are usually not needed. |
|
What is the treatment? |
| |
Today a variety of options are available for the management of pterygium, from
irradiation, to conjunctival auto-grafting or amniotic membrane transplantation, along
with glue and suture application. As it is a benign growth, pterygium typically does not
require surgery unless it grows to such an extent that it covers the pupil, obstructing
vision or presents with acute symptoms. Some of the irritating symptoms can be
addressed with artificial tears. However, no reliable medical treatment exists to reduce
or even prevent pterygium progression. Definitive treatment is achieved only by surgical
removal. Long-term follow up is required as pterygium may recur even after complete
surgical correction. |
|
What are the surgical options? |
| |
Conjunctival auto-grafting is a surgical technique that is effective and safe
procedure for pterygium removal. When the pterygium is removed, the tissue that covers
the sclera known as the conjunctiva is also extracted. Auto-grafting replaces the bare
sclera with tissue that is surgically removed from the inside of the patients upper eyelid.
That self-tissue is then transplanted to the bare sclera and is fixated using sutures,
tissue adhesive, or glue adhesive.
Amniotic membrane transplantation is an effective and safe procedure for pterygium
removal. Amniotic membrane transplantation offers practical alternative to conjunctival
auto graft transplantation for extensive pterygium removal. Amniotic membrane
transplantation is tissue that is acquired from the innermost layer of the human placenta
and has been used to replace and heal damaged mucosal surfaces including successful
reconstruction of the ocular surface. It has been used as a surgical material since the
1940s, and has been shown to have a strong anti-adhesive effect.
Using an amniotic graft facilitates epithelialization, and has anti-inflammatory as well as
surface rejuvenation properties. Amniotic membrane transplantation can also be fixated
to the sclera using sutures, or glue adhesive.
Amniotic membrane transplantation with Tisseel glue application and Mitomycin-C has
shown excellent cosmetic outcomes with a surface free of redness, stitching, or patches,
which makes the ocular surface suitable for vision correction surgery sooner. |
|
What are the outcomes? |
| |
Most pterygia cause no problems and do not need treatment. If a pterygium affects
the cornea, results are usually good after it is removed.
|
|
What are the complications? |
| |
Recurrence
Corneal scarring
Corneal perforation
Strabismus
Non-healing epithelial defect (esp with mitomycin C)
Scleral melt (esp with mitomycin C) |
|
What is the time course? |
| |
People with pterygium should be seen by an ophthalmologist each year, so that
the condition can be treated before it affects vision.
Call for an appointment with your ophthalmologist if you have had a pterygium in the
past and your symptoms return. |
|
What is the expense? |
| |
The expense depends upon the grades of treatment. |